
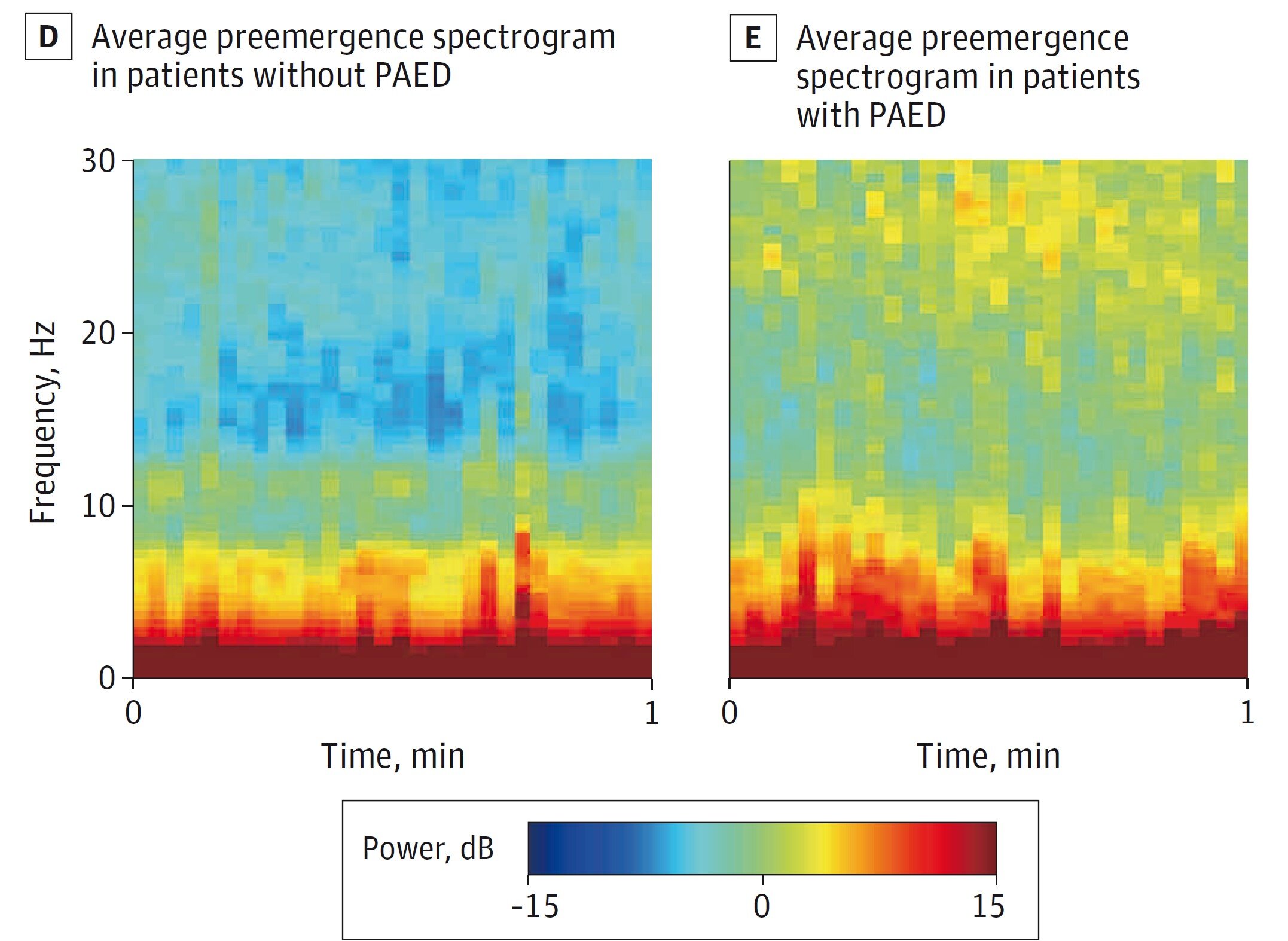
The average pre-emergence spectrograms recorded during research show that contrasts between children who have undergone (right) or who have not undergone (left) Paed. For official reference, please consult 3D figures, E in the study. Credit: Miyasaka, and. al., Jama Pediatrics
The results of a randomized controlled clinical trial in Japan among more than 170 children aged 1 to 6 years who have undergone surgical intervention show that by using EEG readings of brain waves to monitor unconsciousness, an anesthesiologist can considerably reduce the amount of anesthesia administered to induce in complete safety and maintain the anesthetized state of each patient.
On average, patients have experienced significant improvements in several postoperative results, including faster recovery and reduced incidence of delirium.
“I think that the main point to remember is that in children, using EEG, we can reduce the amount of anesthesia that we give them and maintain the same level of unconsciousness,” said the co-author of the study Emery N. Brown, Edward Hood Taplin Professor of Medical Engineering and Computational Neuroscience and Anesticist Massachusets. The study appears in Jama Pediatrics.
Yasuko Nagasaka, president of the anesthesiology at Tokyo Women’s Medical University, a former Brown’s colleague in the United States, designed the study. She asked Brown to train and advise the main author Kiyoyuki Miyasaka from St. Luke International Hospital in Tokyo on how to use EEG to monitor unconsciousness and adjust the dosage of anesthesia in children.
Miyasaka was then anesthesiologist for all trial patients. Participation in anesthesiologists not involved in the study was always on site to supervise.
Brown’s research has shown that the level of consciousness of a person under a particular anesthetic drug is discernible from models of their brain waves. The cerebral waves of each child were measured with the EEG, but in the control group, Miyasaka joined the protocols for the dosage of standard anesthesia, while in the experimental group, he used the EEG measurements as a dosage guide.
The results show that when he used the EEG, he was able to induce the desired level of unconsciousness with a concentration of 2% of Sevoflurane gas, rather than the 5% standard. Maintaining unconsciousness, on the other hand, has only required a concentration of 0.9%, rather than the 2.5%standard.
Meanwhile, a distinct, blind researcher, namely whether EEG or Standard protocols have been used, have evaluated children for the “delirium of emergence of pediatric anesthesia” (PAED), in which children sometimes wake up from anesthesia with a set of side effects, in particular the lack of ocular contact, non-inconstancement, non-consciousness, Movements not purpose.
Children who have received a standard anesthesia dosage reached the paed threshold in 35% of cases (30 out of 86), while children who received a dosage guided by the EEG reached the threshold in 21% of cases (19 out of 91). The difference in 14 percentage points was statistically significant.
The authors reported that on average, the patients guided by the EEG had respiratory tubes removed 3.3 minutes earlier, emerged from anesthesia 21.4 minutes earlier and were returned post-suction care 16.5 minutes earlier than patients who received anesthesia according to the standard protocol. All these differences were statistically significant. In addition, no children in the study has never read during surgery.
The authors noted that the faster recovery in patients who received anesthesia guided by the EEG was not only better medically, but also reduced health care costs. Time in post-acute care in the United States costs around $ 46 per minute, so the average time reduced by 16.5 minutes would save around $ 750 per case.
The sevoflurane is also a powerful greenhouse gas, noted Brown, so reducing its use is better for the environment.
In the study, the authors also present comparisons of EEG children’s recordings in witness and experimental groups. There are notable differences in the “spectrograms” that have drawn the power of the frequency of individual brain waves, both as a child, undergoing surgery and while they were approaching the emergence of anesthesia, said Brown.
For example, among children who have received a dosage guided by EEG, there are high power strips well defined at around 1 to 3 hertz and 10–12 Hertz. In children who have received a standard protocol dosage, the entire frequency range, up to around 15 Hertz, is at high power. In another example, children who have known Paed showed higher power in several frequencies up to 30 Hertz than children who have not experienced Paed.
The results also validate the idea that monitoring brain waves during surgery can provide anesthetists with usable advice to improve patient care, said Brown. The training in reading EEGs and the guidance administration can be easily integrated into the continuous hospitals, he added.
In addition to Miyasuka, Brown and Nagasaka, Yasuyuki Suzuki is co-author of the study.
More information:
Tituration guided by the EEG of Sévolfurane and the delirium of emergence of pediatric anesthesia, Jama Pediatrics (2025). DOI: 10.1001 / Jamapediatrics.2025.0517
Supplied by the Massachusetts Institute of Technology
Quote: In children, EEG conscience surveillance can safely reduce anesthetic use (2025, April 21) recovered on April 21, 2025 from
This document is subject to copyright. In addition to any fair program for private or research purposes, no part can be reproduced without written authorization. The content is provided only for information purposes.

{kind=link}